
What is Panic Disorder? Exploring Symptoms and Therapeutic Solutions
TL;DR
Panic disorder is more than just having panic attacks. It's a cycle driven by catastrophic misinterpretation of anxiety's physical symptoms, where racing hearts get read as heart attacks, and dizziness gets read as fainting. That fear triggers more anxiety, which intensifies the symptoms, which deepens the fear. The avoidance behaviors and safety signals people use to cope only keep the cycle fed. The good news is that cognitive-behavioral therapy has decades of research behind it and directly targets both the distorted thinking and the avoidance maintaining the disorder. Through panic disorder treatment using interoceptive exposure, situational challenges, and gradual removal of safety behaviors, clients learn to approach anxiety rather than flee from it. In doing so, they take away its power.
Panic Disorder: When Fear of Anxiety Becomes the Problem
It is ROUGH out there for people with panic disorder. Folks with panic disorder experience frequent rushes of anxiety that seem to go from 0 to 100 in seconds. They can be so intense that people often think they are dying or having a heart attack, going to faint, going to “lose control” of their bodies, or going to “go crazy.” There are lots of different physical symptoms that people might experience during a panic attack, and all are related to anxiety but interpreted as dangerous. In fact, panic disorder is sometimes characterized as “fear of fear” because it is the symptoms of anxiety and what they might mean that are the primary fear.
Beyond the panic attacks themselves, people with panic disorder are also very concerned about avoiding future panic attacks. Since they are so scary and are interpreted as dangerous, it makes sense that some folks would do everything they can to avoid having one again. This then leads to avoidance of situations or places where panic attacks have occurred before. For example, in the grocery store or while driving. When they believe they are having a panic attack, folks usually try to escape the situation they are in. After that, they might call a loved one for reassurance or go straight to the emergency room (ER) in case they are having a medical issue.
All these behaviors can lead to extra costs, like getting groceries delivered or medical bills from going to the ER. It also makes their lives so much smaller. Over time, they feel they can’t go to more and more places or do certain things. For some, it can even lead to developing agoraphobia and becoming homebound.
What Even Is Anxiety?
To understand panic, it’s important to first understand anxiety. According to cognitive-behavioral models of anxiety, it is the perception of danger that then leads to activation of the fight or flight response in the sympathetic nervous system. Phew, that’s a long sentence. Let’s break it down.
Anxiety does not simply occur whenever you are in danger. There are countless stories of people being in incredibly dangerous situations and not realizing it. There are also the same number (maybe more) of stories involving people who are in no danger of bodily harm, and yet, they are very afraid. Think of it like a very imperfect alarm system. For some people, their alarm system is overly sensitive and triggers when there is no danger. That’s what it’s like to have an anxiety disorder.
Once the alarm is set off, the body moves into action. You may have learned in school that there are two branches of the autonomic nervous system (the part of the nervous system responsible for automatic, or involuntary, functions). One is the sympathetic nervous system (SNS), which is responsible for the fight or flight response, and the other is the parasympathetic nervous system (PNS), which brings the body back into a rest state and activates functions like the digestive system. When the SNS is activated, this brings about physiological arousal that is meant to prepare our bodies to either fight the threat or flee back to safety.
Activation of the SNS involves (but is not limited to) the following:
Cardio: Increased heart rate and blood pressure, to pump more oxygen to the muscles
Vision: Enlarges pupils to let in more light and improve vision
Some people note that their eyes hurt or are particularly sensitive to light during a panic attack
Respiratory: airway muscles relax to bring more oxygen to the lungs. Breathing gets faster as well, again to bring in more oxygen so the blood can bring it to the muscles and brain.
Digestion: Digestion is considered unnecessary when facing a threat to our safety, so all digestive processes slow to divert the energy elsewhere.
Activity in the stomach and intestines slows, sometimes causing stomach aches, nausea, diarrhea, or constipation
The bladder relaxes (sometimes resulting in incontinence when extremely fearful)
Salivation is inhibited (slowed down)
Liver: Activates energy stores and converts them to glucose, which can be used more readily.
Muscles: muscles often tense to prepare for action, sometimes causing trembling or shaking
Sweat: stimulates sweat production to prepare for cooling you down when you run or fight.
Our bodies are really good at this. Fear is a normal, physiological response. Humans developed this to keep us safe. That is the purpose of anxiety. And remember, the fight or flight response only arises when we perceive danger.
What Is Panic Disorder?
Now that we know about anxiety and the fight or flight response, I can talk about panic. With any anxiety disorder, there is typically fear around a specific theme. For social anxiety, the fear is negative judgment from others. For panic disorder, the fear is of the physiological symptoms of anxiety themselves. This is why panic disorder is dubbed “fear of fear.”
The Panic Cycle
Panic disorder can be broken down into three components that all feed into each other in a negative cycle. These components are physical symptoms, thoughts, and behaviors. The physical symptoms of anxiety I outlined above. The thoughts component refers to how we think about, or interpret, those physical symptoms. People with panic disorder will interpret one or more of the symptoms of anxiety as dangerous or life-threatening. For example, an increased heart rate is interpreted as a sign of a heart attack. These catastrophic interpretations then increase anxiety, which then makes the physical symptoms worse, which strengthens the catastrophic thinking, and so on, until a panic attack ensues. This is the panic cycle: a physical symptom arises and is perceived as dangerous, increasing the intensity of the physical symptom, which is perceived as more dangerous, etc.
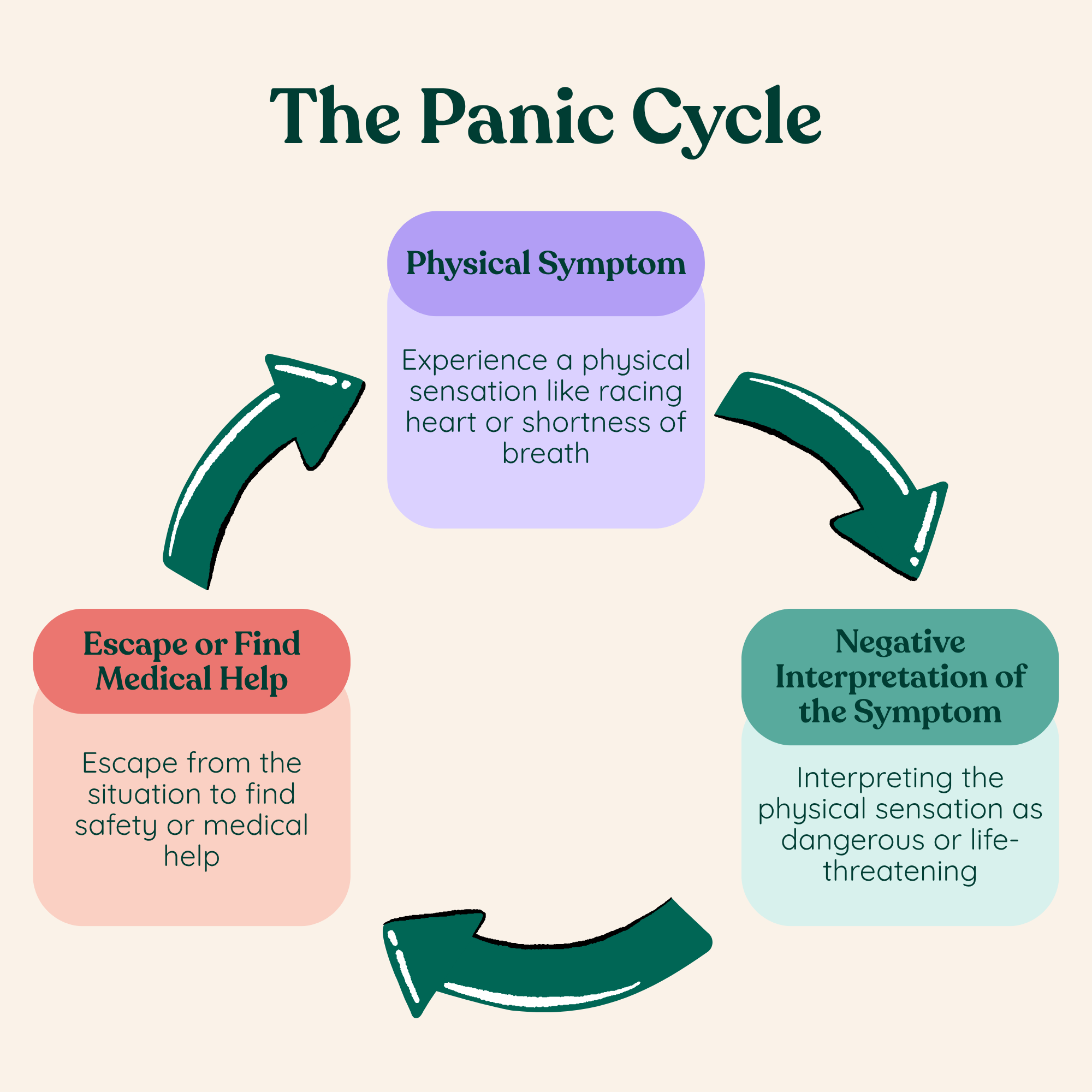
The final piece is behavior. In panic disorder, behavioral responses to those physical symptoms often involve escaping the situation and seeking reassurance from a loved one or seeking medical care. People with panic disorder often have frequent visits to the ER because they frequently have panic attacks in which they believe they are having a medical emergency and need help. These behaviors further communicate to yourself that you are in danger. After all, if you were totally fine, you wouldn’t be beelining to the ER, would you??
Avoidance in Panic Disorder
Because the panic attacks are so aversive and because they are seen as dangerous, people with panic disorder tend to begin structuring their lives around panic. Between panic disorders, they are very concerned about avoiding another panic attack or trying to ensure they can get help if one happens. At Leap Counseling, I’ve witnessed several ways people typically do this:
Avoidance of situations that cause physical symptoms
Since the core fear is of the physical symptoms of anxiety, they will avoid situations or activities that elicit those symptoms
Examples include: exercise (especially cardio), consuming caffeine, using nicotine, consuming alcohol or drugs, or being in hot environments
Avoidance of places where an attack has happened before
It could be anywhere, but avoidance is more likely in places where panic attacks have happened more than once or in places that are not visited frequently but where a panic attack had previously occurred.
The expectation is that a panic attack will happen again if they go back.
Avoidance of places or situations where escape or getting help would be difficult
Since there is a belief they are in danger, they avoid places where they could not easily get help.
There is also a strong feeling or need to escape, driven in part by the fight or flight response itself, during panic attacks. So, folks will ensure they do not go places that they could not easily escape from.
Examples include: being in the middle of the aisle in a lecture hall or movie theater, away from the door; public transit; places that are too open and far from other people; in a crowd; in line (or a queue, if you’re British)
Avoidance of situations in which having a panic attack would be embarrassing
Being in a crowd, at a party, etc.
Safety signals
These are items or people that create a sense of safety if not in a “safe zone.” They may be related to preventing a catastrophic outcome (like a water bottle to prevent choking), or they may be more superstitious in nature.
People with panic disorder often are afraid to leave the house or go somewhere not deemed “safe” alone. They may have one or two people with whom they will go to new or feared locations.
Other examples of common safety signals are: water bottle, cell phone, and as-needed (PRN) medications such as Xanax. Often, folks will not leave the home without their safety signals. Sometimes they have a specific bag with all of them in it.
What Feeds Panic Disorder?
With a CBT approach, we don’t need to try to dig down to some supposed deep-seated psychological cause that probably is related to your mother. The science shows that it’s more important to find out what is maintaining, or ‘feeding,’ the disorder than to find out its cause (which is actually just some combination of genetic, biological, and environmental factors that we haven’t pieced apart quite yet).
The panic cycle is maintained by two related things: The catastrophic interpretation of physical symptoms of anxiety and the avoidance and safety behaviors. One could say the physical symptoms maintain the disorder as well, but we don’t have direct control over those! If folks could just decide not to feel anxious, there wouldn’t be a problem in the first place.
What about benzodiazepines? They can decrease anxiety through biology. Yes, they can, in the moment. But as a panic disorder therapist, what I’ve discovered about benzos is that they actually function similarly to other avoidance or safety behaviors. It will calm you down, but it actually keeps the underlying problem fed. Other types of medication can help, and it might be beneficial to talk to a psychiatrist about what they recommend for you. SSRIs, for example, can be helpful. However, medication can only do so much. I think of it as something that makes it a little easier to do the therapy work, not as a replacement for it.
So, we have to focus on the things that we have more control over: thoughts and behaviors. Remember that the perception of danger is what causes anxiety, and that the perceived ‘threat’ in panic disorder is physical symptoms of anxiety. Thus, continuing to think of feelings of anxiety as dangerous feeds the panic disorder. Behaviors feed panic in two main ways:
Preventing new experiences that could disprove the fear
Communicating to yourself and to your body that the symptom is dangerous
Allow me to illustrate. Let’s say a woman named Sarah is afraid that if she has a panic attack, she will die unless she gets medical help. So, every time she has a panic attack, she goes to the ER. Is she ever going to know what would happen if she didn’t go? No, she will never learn new information because she doesn’t allow herself to test it out. She can continue to attribute the fact that she didn’t die to being in the ER. She won’t learn that she never would have died, even if she stayed where she was when the panic attack hit.
Not only does Sarah not learn anything new, but her behavior itself communicates something to her. Humans are a little funny; how we behave actually shapes how we think and what we believe. When Sarah rushes to the ER, she is telling herself, This is dangerous, I am not safe. She is solidifying her belief that a panic attack is a medical emergency. After all, why would she go to the ER if she wasn’t having a medical emergency? (sound familiar?) Acting like something is dangerous makes us think and feel like that thing is dangerous.
What Is the Best Treatment for Panic Disorder?
Hands down, the most effective psychotherapy for panic disorder is cognitive-behavioral therapy (CBT) for panic. This treatment uses specific, focused aspects of CBT that have been found to be effective for panic disorder (we have decades of research on this!). All of the components of treatment are focused on changing thinking and behaviors to disrupt the panic cycle and stop feeding panic disorder. With CBT, folks learn to tolerate and approach anxiety rather than avoid it. The main components include:
Psychoeducation
The client will learn information about panic disorder, the panic cycle, CBT, and how and why CBT therapy works
Interoceptive exposure
Interoception means the ability to perceive internal physical signals from the body, such as racing heart. Interoceptive exposure involves intentionally bringing on the feared physical sensations. For example, rapid heart rate might be brought on by running in place. Over time and repetition, the physical sensation is separated from the anxiety. While it may still be uncomfortable, it is no longer feared.
Removing safety signals and exposures to avoided situations/places
To really test those beliefs about safety, clients intentionally face their fears by putting themselves in previously avoided situations without their safety behaviors or safety signals. This empowers the client with new information about not only whether the world is as dangerous as they thought, but also about what they can handle. I always say that people are way more courageous than they think!
Challenging distorted thinking patterns

Through the process of testing fears through exposure, clients will also learn information about anxiety and panic that will allow them to challenge their beliefs. Clients learn to identify distorted or unhelpful thinking patterns related to anxiety and challenge those thoughts through different strategies, such as examining the evidence for and against the thought.
Overall, the goal with panic disorder treatment is to change the client’s relationship to anxiety and panic. Instead of something to be feared and avoided at all costs, clients can learn to welcome anxiety (and, yes, panic, too!). This is called changing from an avoidance orientation to an approach orientation to anxiety. By intentionally approaching anxiety, its power is taken away. It becomes less a huge scary monster and more a tolerable nuisance.
Want to Stop Structuring Your Life Around Panic? Online Panic Disorder Treatment in Wauwatosa, WI, Can Help
If panic attacks have been shrinking your world, panic disorder treatment can help you stop avoiding and start living again. CBT is one of the most well-researched treatments in mental health, and it works by targeting the exact cycle that's been keeping you stuck.
Leap Counseling and Consultation is a Wisconsin-based solo therapy practice led by Dr. Johanna Wood, who specializes in OCD and anxiety disorders, including panic disorder. Dr. Wood provides personalized, evidence-based CBT treatment designed to help clients break the panic cycle, challenge catastrophic thinking, and gradually face the situations and sensations they've been avoiding so that anxiety stops calling the shots. Getting started is simpler than panic wants you to believe:
Reach out to discuss your unique situation and schedule a free 15-minute consultation
Work one-on-one with an experienced panic disorder therapist in Wauwatosa who understands the anxiety behind it
Begin changing your relationship with anxiety, from something to be feared and escaped, to something you can face and tolerate
Other Services Leap Counseling Offers in Wisconsin & All PSYPACT States
Panic disorder has a way of making the world feel smaller and smaller until even leaving the house feels like a risk not worth taking. Therapy can help you push those boundaries back out, one step at a time. Many people who work through panic disorder treatment are surprised by how much ground they're able to reclaim and how much more capable of handling anxiety they turn out to be than they ever believed.
Panic disorder is one of several anxiety-related conditions I treat at my Wisconsin-based online therapy practice. Anxiety rarely shows up in just one form, and if other concerns are part of your experience alongside panic, there's room to address those too. I provide therapy for a range of conditions, including OCD, Agoraphobia, Generalized Anxiety Disorder, Social Anxiety Disorder, and Phobias. As a licensed psychologist in Wisconsin and all PSYPACT states, I'm able to meet with clients online across many locations, bringing specialized anxiety care to people who might not otherwise have easy access to it.
No matter how long panic has been running the show, a different way of living is within reach. Browse my mental health blog for more on panic disorder and anxiety treatment, and reach out whenever you're ready to take that first step.
About the Author
Dr. Johanna Wood is a Wisconsin-based clinical psychologist with deep expertise in anxiety disorders, including panic disorder. She earned her PhD in Clinical Psychology from Northern Illinois University and completed her doctoral internship at Rogers Behavioral Health in the OCD and Anxiety Adult Residential Program, where she later supervised clinical staff. She is licensed in Wisconsin, holds PSYPACT authorization, and is an active member of the International OCD Foundation, contributing to national education efforts on scrupulosity OCD.
What sets Dr. Wood apart is that she doesn't just understand anxiety from a clinical standpoint. She knows firsthand what it's like when your own mind and body feel like the enemy. Having personally navigated the intrusive thoughts and anxiety spiral of relationship OCD, she understands the exhausting cycle of fear, avoidance, and the desperate search for safety that defines anxiety disorders like panic disorder. Her own ERP treatment taught her that the only way through anxiety is toward it. A "leap of faith" that she now helps her clients take, whether they're dealing with panic, OCD, or both.
That blend of rigorous clinical training and lived experience shapes the compassionate, no-nonsense approach she brings to CBT-based anxiety treatment at her Wisconsin-based online practice.